The Disease Control Priorities Project has a striking feature article about fistula and maternal mortality
… across much of the less developed world, fistula is an ordinary hazard of childbirth for many women and a permanent blight on countless lives. In those countries, obstetric fistula overwhelming results from obstructed labor, which occurs when the baby cannot pass through the mother’s birth canal because it either does not come head first or is too large for her pelvis. In the developed world, prompt medical intervention, often including Caesarean section, permits a delivery safe for both mother and child. But thousands of times each year in poor countries, birthing women receive no such aid and their labor is a futile agony lasting up to five days, with uterine contractions constantly forcing the baby, usually head first, against unyielding pelvic bone.
Long before the mother’s torment ends, however, the unremitting pressure kills the child. It also cuts off the blood supply to the soft tissues of her vagina and other organs trapped between the baby’s skull and her pelvis. Eventually these tissues also die, forming one or more fistulas, and the baby’s head softens sufficiently for the stillborn child to pass from her body. Should she survive, the mother soon finds urine, feces or both leaking unstoppably from her vagina. In about a fifth of cases, the woman also suffers nerve injury that can cause a condition called footdrop, which prevents normal walking. Constant contact with urine or feces irritates and infects her skin and other tissues. Her kidneys, bladder, or other nearby organs may also be damaged. Her menstrual periods may stop, rendering her infertile.
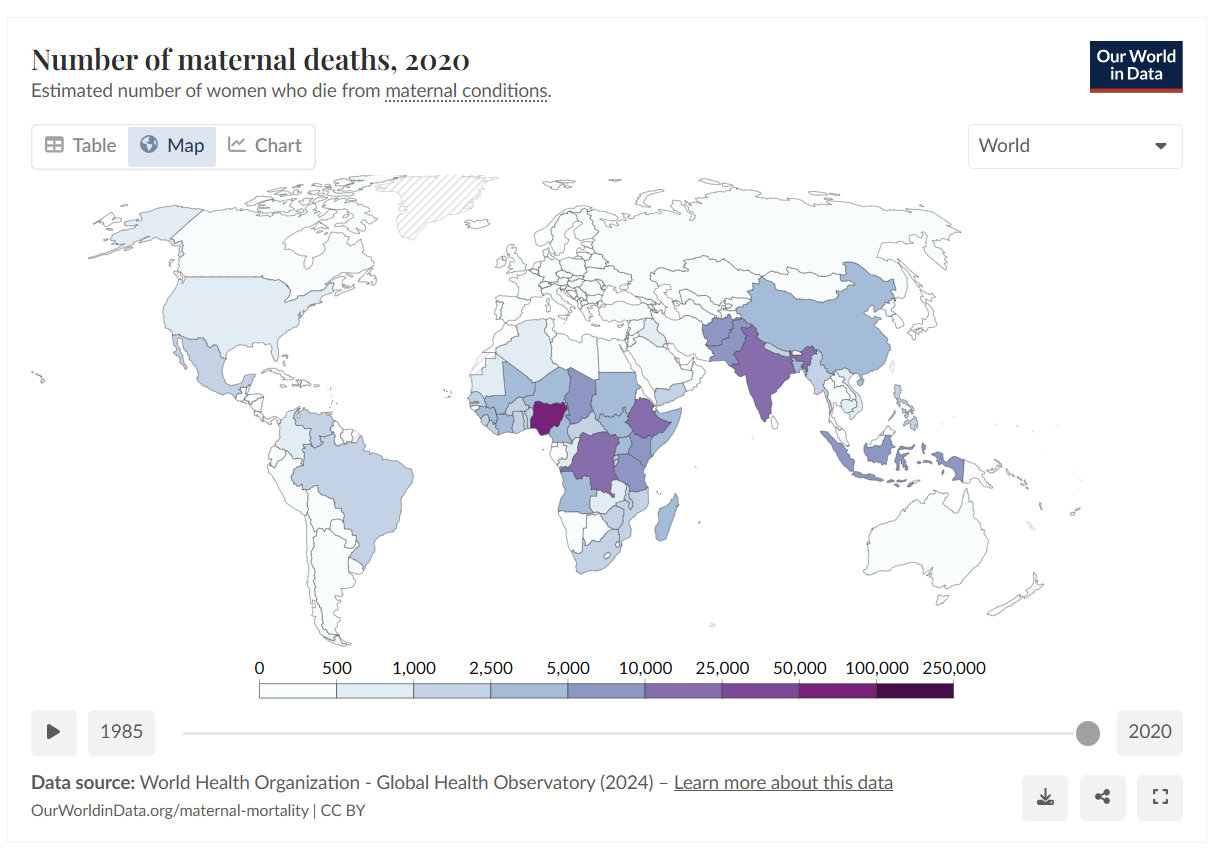
The stark difference between the experience of mothers in the developing and developed worlds explains one of the greatest discrepancies known in health statistics, that between the rates of maternal mortality in rich and poor countries—a gap that constitutes “one of the most neglected issues of social injustice in the world today,” according to Wall and co-authors.17 Only 1 percent of the more than half a million maternal deaths each year happen in developed nations. In Northern Europe and North America, 11 women die for every 100,000 live births and a woman’s lifetime chance of dying because of pregnancy is 1 in 4,000. In Africa, that risk has been estimated at 1 in 14,18 and in some of the poorest parts of the continent, where over a thousand women die for every 100,000 live births, at 1 in 7.19
… A number of facilities, most prominently the renowned Addis Ababa Fistula Hospital, in Ethiopia, repair thousands of fistulas each year at a cost of about $450 for each operation and related care.26 But still, the number of women suffering the disability and indignity continues to grow, creating a backlog that by some estimates would take centuries to clear, but which others believe could, with appropriate effort, be managed in a decade. And given the limited funds available for maternal care overall, experts differ on how to balance resources between prevention and treatment. In the opinion of Dr. Yifru Berhan, an obstetrician in the Ethiopian town of Hawassa, for example, “it’s unfortunate that we have hospitals to manage the complication but not to prevent the complication.”27
(Declaration of interest: my partner works for Marie Stopes International, whose slogan is “Children by choice, not by chance”. Their work to provide women with access to sexual health services including contraception and abortion, enables women to choose when and whether they want to have children, enabling them to avoid pregnancy when they are very young, to avoid having too many children and to increase the spacing between children, all of which are important ways to prevent this kind of complication from pregnancy and childbirth.)





5 responses to “Fistula, and maternal mortality”
This is a tragic problem, but I find myself being struck by your “declaration of interest.” I assume the choice does not pertain to that of the pre-born baby, who we can assume, like when you were pre-born, would want to be brought to term, no matter the circumstances of the conception?
The MSI has exemplary goals, but it chooses evil to achieve the good. In this case, besides taking human life–which is serious in and of itself–it teaches African men not to the concerned about the consequences of their actions. You might argue that they are not concerned now, and thus make life difficult for African women and their children. Yet it is hard to see how removing men from responsibility of their actions, as well as a major impetus to learn self-discipline, can make the situation any better.
One might add: Why do unwanted pregnancies, festulas, etc., persist in developing countries that embrace abortion and abortifacients (like the Pill)? And why are such policies always directed at black communities, in the the developed and undeveloped world?
[…] until I read this article from the Disease Control Priorities Project, which I learned about on Owen’s blog. Here’s an excerpt (be warned, it’s pretty graphic): In developed countries, fistulas […]
Barry – Unlike you, I don’t believe that we have any moral obligations to abstract “potential future human beings”. Your phrase “when you were pre-born” has no meaning – before I was was a human being there was no “you” to be “pre-born”, and it follows that it is a mistake to impute choice, or preferences such as “would want to be brought to term”.
So when the baby kicks in response to the knife being jammed into her head–maybe it just cuts off an ear on the first try–do you console yourself by saying that she is only a “potential future human being”? (This was your term, not mine.) Also, I’d warn you about the slippery slope you are now occupying. How old were you when you were able to impute choice? Did you only exist in the abstract until that point, and should the right to life start after that point?
A broader element of this issue is that of the principal-agent. In the relationship between the people and the social system, the people should be the principal, and the social system the agent. It should not be the other way around. Those who consider abortion a solution impose violence to make the people conform to a faulty social system, when the social system should adjust to the dynamics of the human population. It reminds me of the Keynesians, or the Soviets, who needed to force people to conform so that their systems would work like they were supposed to on paper.
Having in the past had some pretty strenuous debates on the issue of abortion on my own blog (e.g. here, I have concluded with regret that there’s insufficient common ground for useful discussion between on the one hand those who are unable to distinguish between a foetus and a human being, or between a “potential” human being and an actual one, and on the other hand those who believe that women should have control over their own bodies without being limited in that freedom of action by others, generally men, whose stake in the consequences of their decisions is negligible or non-existent. I have also concluded that participants in this debate have a duty to declare where they are coming from — it whether their views are governed or coloured by adherence to religious doctrine, or whether they have arrived at them by purely secular moral analysis. I write (obviously) as an atheist.
Brian
http://www.barder.com/ephems/