Save the Children has today published a new report, No Child Born to Die: Closing the Gaps. It is accompanied by an excellent new video which is well worth two and a half minutes of your time:
Eight million children die each year before their fifth birthday, mainly of easily preventable and treatable diseases. About 1.6 million children under five die of pneumonia, and 1.3 million of diarrheoal diseases. These diseases two account for three times as many deaths as malaria and HIV combined.
Save the Children are right to highlight the success of vaccines to combat these preventable deaths. And they are right to emphasize the need for donors to give enough money to the Global Alliance for Vaccination and Immunization (GAVI) to enable it to fund more vaccinations. GAVI says that it needs $500m a year more to enable it to provide existing and new vaccines. Donors should come to the London meeting in June 2011 ready to pledge it.

I am not however persuaded by SCF’s call to “bring down vaccine prices”. They should be careful what they wish for. If prices for vaccines used in developing countries are too low, pharmaceutical companies are less likely to develop new vaccines for diseases predominantly in developing countries and less likely to manufacture such vaccines in large quantities. If anything, we should be trying to sustain vaccine prices at a reasonable level which provides a decent return to vaccine manufacturers who get involved in these markets. I have no quibble with any measures to reduce the actual cost of those vaccines (eg by reducing unnecessary regulation or by reducing uncertainty) but it would be unwise of donors to use their monopsony purchasing power to make the production of vaccines for developing countries more unattractive for pharmaceutical companies. We want vaccines to be affordable, but it is likely that subsidies are a better way for donors to do this than by limiting the economic value of this market.
The SCF is also wrong to call for an end to health worker recruitment by developed countries from developing countries. First, we do not know whether this kind of migration reduces or increases the number of health workers in developing countries. There is a positive relationship between the number of African health workers inside a particular country and the number of health workers from that country working abroad, which suggests that the opportunity to emigrate may play a role in recruiting more people to the health professions, more than compensating for the number of people who end up emigrating. Second, this kind of regulation is not an effective way of influencing the migration choices of skilled workers: we should instead be asking how the health system would need to change for them to want to stay. Third, this treats health workers as a human resource not as human beings. Why should they be denied the opportunity to make their own lives better, if that is what they choose to do?
Not every country is constrained by lack of money; but some clearly are. Ethiopia, where I live, is a case in point. Health spending per person is about $30 per person per year; and of that, the government spending is about $17 per person. With a committed Minister, the government has achieved an extraordinary amount with very little money, especially through the introduction of health extension workers, but they could clearly do so much more if they had more money to spend. Save the Children is absolutely right to call for long-term commitments of funding for health systems to enable governments to increase these basic health services.
Well done to Save the Children for starting this campaign: it is a global scandal that so many children die of easily preventable and treatable diseases. As Save the Children rightly says, we should mobilise funding for vaccines and improve the provision of long-term funding for health systems.





16 responses to “Born to shine”
[…] Born to shine AKPC_IDS += "10196,";Popularity: 50% […]
Owen – interesting piece, one nitpick even though I agree with your main point on the brain drain:
“Why should they be denied the opportunity to make their own lives better, if that is what they choose to do?”
Most, if not all of these people will have been trained in schools heavily subsidised by government/donor money, right? Surely it is then more reasonable to say, “No, you don’t get to get on the next flight to the UK, you have to work for us for X years first.”
Or, given the massive rate of return African doctors can make on their degrees in the West, how about a tax on subsequent earnings for X years? If governments are paying for it, then they have the right to a return on that investment.
Matt
That seems to me primarily a matter between governments and their citizens. It does not justify rich countries blocking the advancement of African health professionals.
Owen
I do think mass communications could also really help, and for less money and less at risk of driving long-term dependency: have you seen the work of Development Media International? http://www.developmentmedia.net/success.html
During my VSO time in Nigeria (2008-2010), I was surprised how many people didn’t boil water (even if they had the means) or would sell donated mosquito nets, or would prefer to use fields in built-up areas rather than toilets.
When someone – any age – died, the explanation would usually be ‘they were sick’. The cause was rarely sought and therefore very little visibility of what it was and how it could be prevented.
But virtually everyone listens to the radio.
Owen great piece (as usual) and I would like to add to the arguement for allowing individuals always being allowed to make their lives better through migration – and not just within the health field.
Matt in terms of looking at what advantages come to real people on the ground through individuals being able to migrate perhaps look at Owens previous post showing how remittances from overseas workers outstrip government aid, arrives quicker after disasters such as Tsunamis etc, and probaly goes to real people in real need rather than being caight up in bureacratic process etc.
Good point – there should be no blanket bans. Although, given the absolutely massive wage differences, even reasonable schemes in poor countries to keep their professionals around a little longer are unlikely to be viable without the help of the rich countries that demand these workers.
It’s a little bit like saying that the drug flow from Mexico —> US is purely a matter between the Mexican government and its citizens.
Julian,
I’m 100% in agreement that the default position should be free movement – the benefits are clearly there. However, it is unfair for governments in poor country to spend resources investing in people who will then leave, with no guarantee of a return on that investment, and I believe enforcing a guarantee will sometimes require action on the part of countries that attract these health workers.
Matt
A more honourable position would be for rich countries to pay more for the training of health professionals in developing countries.
We can’t seriously say that we want to encourage and reward health professionals in developing countries by singling them out for special obstacles which prevent them from earning their living abroad, if that’s what they choose do to.
The evidence on this is quite striking: African countries which export a lot of health professionals have more health professionals at home too.
This really is one of those well-meaning NGO policies which hasn’t been properly thought through.
Owen
Matt,
“It’s a little bit like saying that the drug flow from Mexico —> US is purely a matter between the Mexican government and its citizens.”
But the flow of illegal narcotic drugs from anywhere into the US does serious and measurable harm to American citizens, and is therefore a legitimate issue for preventive action (however ineffective or counter-productive in practice!) by the US government. By contrast, the flow of health workers from developing countries into developed western countries actively benefits both the receiving countries and the migrating workers; and as Owen shows, it benefits the exporting countries too (by encouraging their people to train and practise as health workers, not all of whom emigrate, and through the remittances sent home by those who do). To try to reduce this mutually beneficial flow by imposing taxes, banning or limiting the recruitment of health workers from developing countries, or otherwise, seems likely to be inherently unjustified and to do more harm than good, as Owen suggests.
Isn’t this post also about specialisation? Save the Children is a Child Saving organisation, and they are probably good at it. Perhaps they are not as good at economics or migration policies.
However, these policies are extremely relevant for children. Supposing Owen is right on these policies, how can Save the Children be saved from these kind of mistakes?
It makes me think of the HIV/AIDS projects where well-meaning doctors start micro credit schemes for HIV/AIDS patients to start economic activities.
Owen and Brian,
Sorry to harp on about this. I understand the basic concept and results of the Clemen’s paper, which I think is innovative and convincing (but, I believe, currently the only piece of rigorous evidence on this specific topic at all).
But let’s be clear on his results: while there is a positive partial correlation between health workers abroad and at home, this positive relationship *vanishes* for the more robust instrumental variables estimations (Table 2). This means that emigrating health workers are perfectly displaced (but that there is no virtuous cycle, 10 health workers are replaced by 10 health workers, not by 15). The same holds for nurses (Table 3).
This means that African health care worker stocks are indifferent to emigration, and we don’t know why (Clemens himself says we can’t tell if it is due to encouraging people to train or through more aggressive work on the government’s behalf, in a complex world of cross-country regressions analysis, we’ll never be able to tell). This is pretty encouraging, and it means we shouldn’t be afraid of emigration.
For all my nitpicking, I do believe the priorities *are* making life easier at home for these health professionals, *not* punishing them, and that includes more donor funding. But that doesn’t mean that recipient governments shouldn’t consider ways to capture some of the massive *private* (income gain and the remittances back home) surplus generated by this emigration, given that it is generated by the public purse in the first place. This indeed could be an awful idea, but we really don’t know enough about how sharp the elasticity of demand for training is – it could be quite robust to small `taxes’ like a requirement to stay home for just a few years.
I’ve met plenty of students from middle-low developing countries who get a high quality education paid for by their home government, but they are required to go home and work it off. This is entirely anecdotal, but I’ve always gotten the sense that the returns to the training are so massive that the price is gladly paid.
Matt
@Matt –
I am not saying that emigration of health workers is an excellent way to strengthen domestic health services. But as you rightly say, such evidence as we have tells us that health worker emigration makes no difference to the number of health workers in the country which they leave. This means that SCF is plain wrong when it says:
On the contrary, as far as we know when health workers leave to take their skills elsewhere this has no effect at all on the number of workers in the health system which they leave behind, and hence does not have the negative effect which SCF claims on child survival or on the health MDGs.
Let me be clear: I’ve no objection to developing country governments considering how they might retain the services of health professionals in whose training they have invested. They might use student loans which are automatically repaid when the doctor or nurse works in the health system, perhaps with a premium for those who work in rural areas; or there might be a contractual agreement. The government should consider this in the context of the broader questions of salary, terms and working conditions. That all seems entirely reasonable. It seems likely to me that they may conclude that the effect of this on recruitment and morale is too high to make it worthwhile, or they may not.
But that is a far cry from what SCF recommends, which is:
I think we can both agree that it is completely legitimate for developing countries to consider contractual or other arrangements to do their best to retain their health professionals, without agreeing with the SCF recommendation that donors should impose a blanket ban on active recruitment of health professionals on whom there is no existing restriction and who want for personal and professional reasons to work elsewhere.
Owen
Owen,
thanks for taking the time to read the new Save the Children report, with which we launched our ‘No Child Born to Die’ campaign this week. I’m pleased that you agree with us that vaccines have an important role to play, as part of a wider package of interventions, provided through a functioning health system, in cutting child mortality rates. And we’re on the same page when it comes to the need for more predictable donor support for recurrent costs in order to bridge the critical shortage of health workers.
You raise a couple of important points, about vaccine prices and health worker migration. I’ll take each in turn:
On vaccines, you’re right that price is not the only consideration. UNICEF, which handles GAVI procurement, will tell you that the quality and predictability of supply matters too, so they’re not simply following a lowest price model in their contracts. It’s also true that the incentives for R&D matter – although from a pharma point of view the scale and predictability of demand for vaccines matters at least as much as price (Something the AMC was supposed to provide, although there are serious questions about how effective it’s really been).
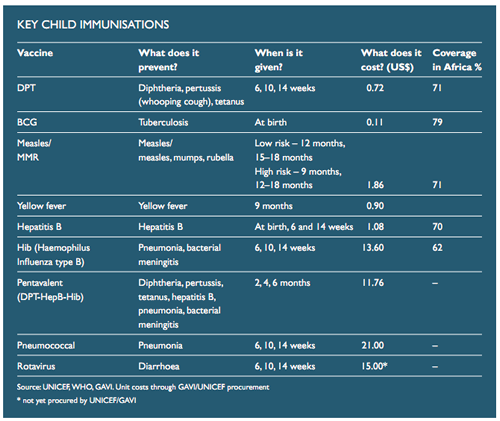
Having said all of this, the prices for rotavirus, pneumococcal and pentavalent remain very high in comparison with the routine vaccines such as DPT and measles ($21 for pneumococcal, against $0.72 for DPT), and explain a large part of GAVI’s unmet funding needs. The recent price fall for pentavalent, for example, shaved hundreds of millions of dollars off the immunisation funding gap. The private sector has a responsibility, as a key GAVI partner, to make these vaccines as widely accessible as possible. GAVI’s own evaluation shows that prices haven’t fallen as much as they expected for the new vaccines (or as far as they need to fall), so this point should be uncontentious. Vaccines are highly profitable, and pharma make good money from their sales in middle- and high-income countries. Price reductions for new vaccines in GAVI eligible countries are feasible, as well as necessary (they would also put further pressure on aid donors to stump up the cash).
On health workers, I don’t believe that we propose blocking migration from developing countries. What we say was (deliberately) more nuanced – we think rich countries like the UK should not actively recruit from countries with critical shortages, as defined by the WHO, and should provide support for those countries so that the push factors are minimised. We recognise that there’s a tension between individual and collective costs and benefits from migration, and that some health workers are best able to apply their skills outside their home country, but the current flow of health workers from Africa to the OECD represents a resource transfer to the rich world. We think the WHO code of conduct on this issue is a good starting point.
Thanks again for engaging on these issues. I hope that we can collaborate over the coming months…
Best, Patrick
@Patrick
Thanks.
On vaccines – we desperately need more incentives for research and development of new vaccines for developing countries, and investment in production capacity to supply those markets with both new and existing vaccines. We both agree that this is partly related to price, and also to predictability.
Vaccine companies are subject to the “hold up” problem – that is, the danger that they invest in R&D and large scale production and are subsequently unable to recover their costs because well-meaning but misguided activists demand that the product is sold at marginal cost. Because they know this is a serious risk in the future, they are less likely to invest in the R&D and production capacity today. The kind of campaign you are running to “bring down prices” adds to that risk, with the unintended (but predictable) consequence that there will be fewer lifesaving vaccines in future, and smaller production for developing countries.
The vaccines for pneumo and rotavirus are more complex than the old DTP vaccine. Their price will fall over time, but it may never be as low as the price of DTP.
So if you are going to claim that “price reductions for new vaccines in GAVI-eligible countries are feasible” you’ll need to produce evidence that the firms are making thumping returns in these markets which should be eroded by driving down the price. What I observe is the opposite, which is that there has been an exodus by private pharmaceutical companies from serving these markets, and a plausible explanation of this trend is that they are driven away by precisely this kind of campaign.
I’m interested in your claim that “the current flow of health workers from Africa to the OECD represents a resource transfer to the rich world”. If you want to think of these people’s lives as “resource transfers” then I think a more appropriate metaphor is that it is an “export” (of skills and services) rather than a “resource transfer”. Many countries – such as Ireland and Norway – have done well in the past by “exporting” the services of their people to plances where they can earn a better return. I dearly hope that you believe that rich countries should dismantle the restrictions which prevent developing countries from exporting other goods and services to rich countries, so I’m not clear why this should be an exception.
But, stepping aside from the dehumanising language of “resource transfers” and “exports”, I also think it is quite wrong to treat people as instrumental pawns to move about for reasons of public policy. If a person from a developing country is able to improve their prospects by getting a better paid job in a rich country, and if there is demand for that person’s services in that country, and if they have no contractual obligation which prevents it, then I think it is quite wrong for you to be arguing that their choice should be restricted because of your view of the wider public policy issues. We have to treat people as more than a means to an end.
I would be against this kind of restriction even if there were evidence – which there is not – that emigration of health professionals reduces the number of health professionals in the system which they leave behind. But since there is no evidence at all that this emigration does any harm, and it is clearly of significant benefit to the individuals concerned, I really think you should reconsider your call for donor countries to try to limit it.
Owen
I love this article.
I see two other possible benefits of health professionals working abroad:
– many migrants send money back to their countries, helping to support their families and communities back home. Though it may not impact directly on flourishing their domestic health care system, it may help increase local prosperity.
– if African health care professionals are anything like Indian ones they often work abroad for most of their professional lives and then move back to their country to “active” retirement, often sharing their knowledge and skill-set before they fully retire.
This is a great research area. Would be good to get some solid economic stats behind it to help promote it positively for Africa’s benefit.
Priya
Owen thanks, and thanks to Save the Children for raising the profile of immunisation needs and this remaining funding gap: the case for greater investment in it is rock solid.
I wanted to add a nuance on the need for complementary investments, which are equally under-emphasised locally and globally, especially in effective sanitation, whose absence is still a source, or at least contributing factor, of at least as many avoidable child deaths as any single vaccine-preventable disease.
So, for example, it is great that there is now a vaccine on the scientific shelf, though alas not yet in most poor communities, to prevent rotavirus, which I see is involved in nearly a third of diarrhoea-related U-5 deaths. But this should not be taken as a “magic bullet”, as compared to the slower, undoubtedly messier but just as powerful dynamics of ensureing that villages are free of open defecation-known as community-led total sanitation in development-speak.
When you see whole villages joyously celebrating reaching the point of being s#i*-free, it gives a different perspective of relative priorities-complementary of course to having vaccines available. (You do not have to look too far afield-the wider availability of anti-retroviral treatment comes to mind-to see that human nature tends to come to see some drugs as substitutes, not complements for basic, but not so easy, prevention measures).
keep up the good work.
Andrew